
by William W. L. Glenn, M.D.
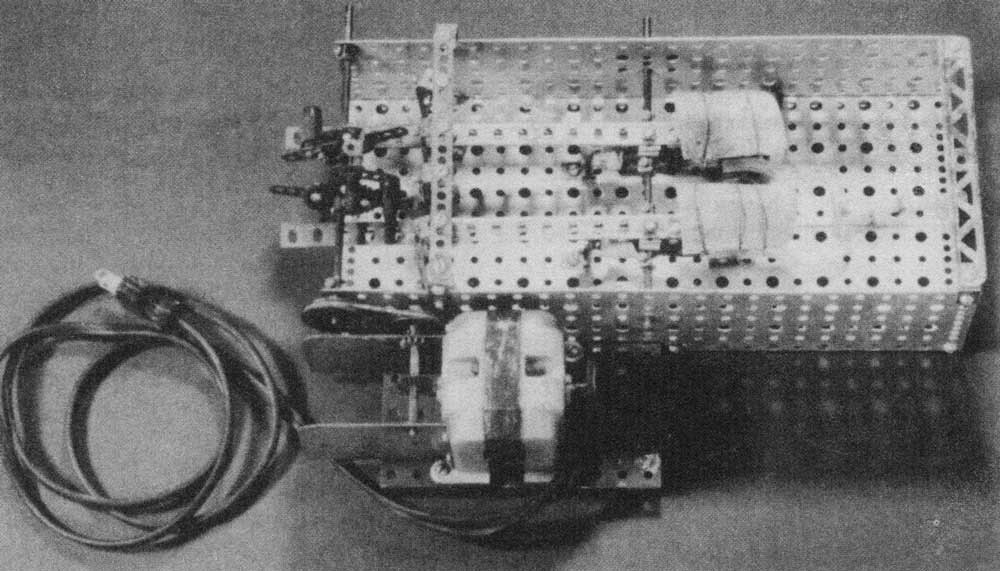
Photograph of a heart pump for by-passing the right heart of dogs, part of a thesis presented to the School of Medicine. Yale University, 1950 hy William H. Sewell, Jr., M.D.
When William H. Sewell, Jr., attended Yale Medical School in the later part of the 1940s, it had long been the policy of the school, at least since 1839, to require its students to prepare a dissertation prior to graduation. This requirement had been reaffirmed when the curriculum underwent a major revision between 1920-25 under the guidance of Dean Winternitz, and the "Yale" plan of medical education evolved. It emphasized that the required dissertation be an "original research." Nearly all students completed a research project during the four years of medical school, but a few who became deeply involved in their projects dropped out of medical school temporarily to complete them. Bill Sewell was one of these students; he had in mind to build an artificial heart.
I do not know when he first got the idea that he wanted to build an artificial heart. It is likely this was when he entered medical school and perceived a practical use for his mechanical skills. He told me that as a child he often played with an Erector set his father bought him. That mechanical things were of continuing interest to him, probably an inborn trait, is shown by the hobby he dedicated much of his spare time to later in life, the building and flying of model airplanes.
Bill's plan was to build an "artificial heart" that could be used in laboratory experiments to study the problems that the cardiac surgeon would encounter repairing intra cardiac defects. By 1948, three milestones in cardiac surgery had recently been reached: in 1938, the successful ligation of a patent ductus by Gross; in 1945, the successful treatment of cyanotic heart disease by Blalock and Taussig; and in 1948, the successful revival of mitral vulotomy by Harken, Bailey, and Brock. All three of these operations were done blindly with the heart functioning. Intracardiac operations under visual control required bypassing of the heart. Gibbon and others had been working for more than 10 years constructing an extracorporeal pump-oxygenator to serve as a substitute heart and lungs during intracardiac operations. When Bill Sewell began his studies, no intra cardiac operation using a pump-oxygenator had been reported, and, indeed, it was by no means clear whether extra corporeal artificial oxygenation of the blood was necessary. Perhaps the patient's own lungs which would not be involved in an operation on the heart could be used· to oxygenate the blood during an intra cardiac procedure. There would then be needed only a pump or a pair of pumps to substitute for the heart. Bill wisely decided to first apply his pump to bypass the right side of the heart.
In some preliminary experiments early in 1948, he found that his initial design which used a roller pump for his artificial heart was not feasible as the small Erector set motor that he would employ did not have sufficient power to propel blood through the rubber tubing. He, therefore, turned to pneumatic power for"propulsion. Pumps of various designs had been used by investigators to perfuse organs, which Bill carefully documented in his thesis, but none were designed to direct the flow of blood through a pneumatically-powered pumping chamber, the direction of flow being controlled by intrinsic valves.
The design of his pneumatically-powered pump was an example of elegant simplicity. It consisted of a tubular glass pumping chamber with' a side arm connected to a compressed air and vacuum source and a rubber bladder made of reinforced Penrose tubing held in place by perforated rubber stoppers. The inflow and the outflow of the pumping chamber were guarded by simple rubber-flap valves made from a toy noise-maker. Blood removed from the venae cavae or the right atrium through a single cannula was drawn into the pumping chamber by suction and driven by compressed air into the pulmonary artery through a glass cannula. A flowmeter based on the Venturi principle was incorporated in the outflow line. The timing of the systole (compressed air) and diastole (suction) was controlled by eccentric cams and weighted arms with vertical blades that occluded and released small rubber tubes (blood pipette tubing was ideal) leading to compressed air and vacuum sources. In most experiments, the pump performed flawlessly.
I had come to Yale in October of 1948, the first appointment of the Chairman of the Department of Surgery, Dr. Gustaf Lindskog, who placed me in charge of the Surgical Laboratories and the embryonic Section of Cardiac Surgery (Cardiovascular). It being required at Yale that all students have a thesis advisor, Lindskog suggested that I work with Bill Sewell, which was a most fortunate circumstance for me. Since this was my first year at Yale, my clinical responsibilities were reasonably light, and Bill was free to work full time on his project. The result was that we spent many hours happily engaged in laboratory experiments. I knew nothing about pumps except what I learned from Bill; my contributions to the project came from my surgical training and lessons in fundamental research gained in Cecil Drinker's physiology laboratory at Harvard. Bill once remarked that he thought I had kept him from "moving ahead too fast", and I suspect that this was also true.
After a number of acute experiments on dogs to work out procedural details and to ascertain that there were no forbidding physiologic or biologic obstacles to right heart bypass, two long-term survival experiments were carried out with all the preparations that we applied to a clinical operation and its post-operative management. Total bypass of the right side of heart for 61 and for 82 minutes was accomplished, with the right ventricle widely open during most of this time. After restoration of the normal circulation, removal of the pump, and closure of the chest, the dogs made an uneventful recovery. Sometime later an elective autopsy revealed no pathologic abnormalities related to the operation. That it was possible to bypass one side of the heart with a mechanical pump for a prolonged period with survival of the animal and that the chamber of the right ventricle could be exposed long enough for deliberate performance of a cardiac operation under visual control had been demonstrated. A preliminary report of these experiments was made at the Surgical Forum of the American College of Surgeons in 1949, and a more formal report followed in Surgery in 1950 (28:474).
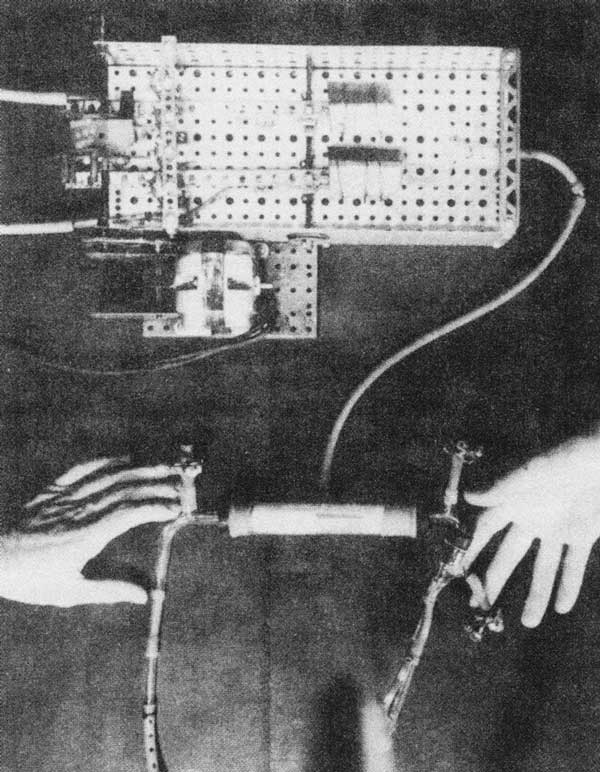
The assembled pump attached to the cam-lever unit driven by a small Erector™ set motor which opens the suction and pressure lines alternately, for the purpose of forcing blood through and out of the pumping chambers. The hand on the right supports the outflow end of the pump and attached pulmonary cannula while the hand on the left supports the inflow end of the pump and the single atrial cannula. In other experiments, the right atrium was isolated by removing the systemic venous return with a single venae cavae cannula.
Bill Sewell returned to his studies and graduated with the class of 1950, receiving the coveted thesis prize for his work. We used his pump in 1951 to study the 'character of coronary blood flow and devise methods for its safe removal from the open heart. In 1952, with a commerciallymade version of Sewell's pump (only one was made) in conjunction with a donor animal to provide oxygenation for the subject animal, experiments on the prevention of air embolism from the open heart were carried out employing electrically induced ventricular fibrillation.
In 1952, the first successful open heart operation with the aid of a mechanical pump was carried out by Dodrill in a patient with pulmonary stenosis. The technique he employed--a mechanical pump and autogenous oxygenation--was the same that we had used earlier in the experimental laboratory. In 1953, Gibbon performed the first successful intra cardiac operation using extracorporeal oxygenation. For a short time it was uncertain if there would be a place for autogenous biologic oxygenation in open heart operations, but as the commercial pump oxygenators improved, it soon became obvious that the latter was the method of choice.
It was not long, however, before Sewell's concept of using a pneumatically-powered pump as an artificial heart was applied to a patient, first in 1964, by DeBakey, using a pump almost identical in design to Sewell's. By creating a left atrium-descending aorta bypass, this was a temporary method to assist the failing left ventricle. It was later applied as a total artificial heart for temporary or permanent replacement of the failed right and left sides of the heart. The first pneumaticallypowered total artificial heart was used as a bridge to transplant by Cooley in 1969. Kolff, working with Jarvik and DeVries, designed a compact implantable pneumatically-powered total artificial heart with which, in 1982, they made the first attempt at permanently replacing the failed biologic heart. Barney Clark, their widely publicized patient, died from multiple organ failure, as did several others who followed. Since then, attention has been focused on the use of unilateral or bilateral assist devices to temporarily replace the failing heart to allow time for spontaneous recovery or procurement of a transplant for cardiac replacement. Results have been remarkably successful considering the extremely poor condition of the patients receiving these devices.
In all of these patients, it was the pneumatically-powered heart, the prototype of which was proved efficient in laboratory experiments nearly 45 years ago, that was used. It is clear, however, that for permanent implantation of an assist device or for a total artificial heart, pneumatic power is impractical. A few years after Sewell worked on his pump, Kusserow in the Department of Pathology at Yale in 1958, designed the first implantable electrically powered artificial heart. In recent years, great progress has been made in the development of electrically powered hearts, particularly by Pierce and his associates. The most successful hearts have been powered by induction from the interior. Pierce believes it likely that by the year 2000 electricity will be the method of choice for powering these devices.
The visionary concept of an artificial heart by a young and talented medical student working in an environment conducive to research and at a time propitious for the development of intra cardiac surgery led to one of the foremost advances in surgery in this century. Bill Sewell built his pump from pieces of a child's Erector set, odds and ends from ordinary laboratory supplies, and dime store items. The total cost was $24.80:
- Glass tube pumping chamber and $2.50 connectors (15x2.8 cm) Valve from "Raspberry" (toy 0.10 noise maker)
- Venous (polyethylene) cannula 0.20
- Arterial cannula (glass) made in lab NC
- Flow meter (200x0.25 cm) glass tubing 5.00
- Brombenzyne (SpG 1.4) 3.00
- Mercury for manometer 3.00
- Silicone coating of cannula NC
- Erector set parts, including motor 9.00
- Eccentric cams 2.00
A recent inquiry revealed that since that time, when the effectiveness of this simple pump was demonstrated, over 200 million dollars in Federal grants have been made to expand and perfect cardiac assist devices and the total artificial heart.
About 1960, Dr. John Blake, Curator of the Division of Medical Sciences of the Smithsonian Institute, approached me for suggestions of new devices used in cardiac surgery appropriate for permanent exhibition at the Institute. Among other things, I suggested Sewell's pump and Gibbon's heart-lung machine. Sewell had preserved his original pump intact and turned it over to the Institute along with a copy of his medical school thesis. Gibbon was contacted, but the "Queen Mary", as his original pump-oxygenator was called, had been dismantled and could not be put back together. Along with Sewell's pump in the exhibit is the LindberghCarrel pump which was built by Charles A. Lindbergh about 1930, for use in Carrel's laboratory for the perfusion of small organs; Lindbergh, trained as an engineer, had hoped to build an artificial heart for use in patients. Lindbergh and Sewell shared the belief that a mechanical device would one day be accepted as a rational substitute for the ailing heart.
C. W. Ohse Professor Emeritus, Yale U. School of Medicine Dept. of Surgery.
Reprinted by permission from The Guthrie Journal 63:1 (Winter 1993)

